Welcome to meidicross the leading medical facility for the health of you and your family.
Welcome to meidicross the leading medical facility for the health of you and your family.

Last updated: June 12 ,2026
Q: What are intravascular treatments in Pune?
A: Intravascular treatments are minimally invasive, pin-hole cardiac procedures performed inside the coronary artery — including IVUS, OCT imaging, Rotablation, and Orbital Atherectomy — to diagnose and treat complex blockages with precision impossible on standard angiography.
Q: When is regular stenting NOT enough for a blocked artery?
A: Regular stenting is insufficient when blockages are heavily calcified, located at a bifurcation, longer than 25mm, or in the left main artery. These complex lesions require advanced intravascular imaging and modified plaque preparation before a stent can be safely and fully deployed.
Q: What is Rotablation (Rotational Atherectomy)?
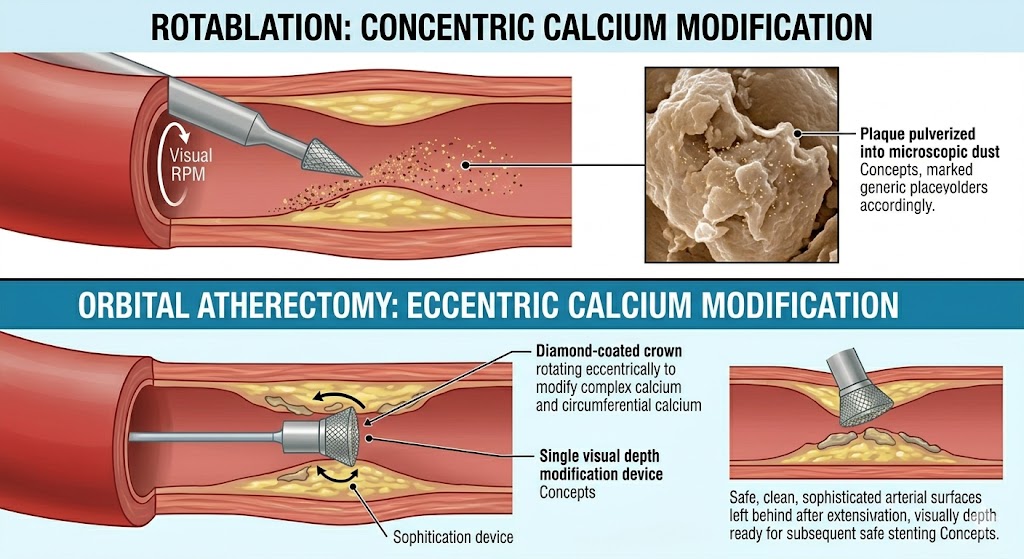
A: Rotablation uses a diamond-tipped rotating burr at 150,000–180,000 RPM to pulverise calcified coronary plaque into microscopic particles. It is used when standard balloons cannot cross or adequately expand a hardened blockage — enabling safe stenting of lesions previously considered untreatable.
Q: Does OCT imaging reduce recurrence after coronary angioplasty in Pune?
A: Yes. Multiple clinical trials confirm that OCT-guided angioplasty reduces in-stent restenosis and stent thrombosis rates compared to angiography-guided procedures alone — directly lowering the probability of a repeat procedure within 1–3 years.
Q: Is advanced intravascular treatment safe for elderly patients?
A: Yes. Advanced intravascular procedures are performed under local anaesthesia, typically through the wrist. Elderly patients tolerate them well. The precision of imaging-guided treatment actually reduces complication risk by ensuring correct stent sizing and placement from the outset.
Intravascular treatments in Pune have entered a new era — and most patients sitting in cardiology waiting rooms have no idea it exists.
For decades, placing a coronary stent meant this: the cardiologist injected contrast dye, watched it flow through the artery on X-ray, identified the narrowing, and inserted a stent based on what that shadow suggested. For simple, short, non-calcified blockages in younger vessels, this approach works well.
But coronary artery disease rarely presents in a simple, cooperative form. Real blockages — the kind seen in patients with decades of diabetes, hypertension, and high cholesterol — are calcified, long, tortuous, or positioned at vessel branch points. They are the kind of lesions that defeat standard balloons, cause stents to under-expand, and account for the majority of repeat procedures performed one to three years after the original intervention.
The solution is not a better guess. It is better information — gathered from inside the artery, in real time, before a single treatment decision is made.
This is what modern intravascular treatments deliver. And at Good Heart Clinic, Pune, they are not a future aspiration. They are the current standard for every complex coronary case that walks through the door.
Not every coronary blockage is equal — and treating a complex lesion like a simple one is one of the most preventable causes of stent failure.
Standard coronary angioplasty with balloon and stent is appropriate for a specific subset of lesions: short, non-calcified, single-vessel blockages in reasonably normal-sized arteries. The moment any of the following features are present, the calculus changes entirely — and advanced intravascular treatment becomes not optional, but necessary.
Calcium deposits within the coronary artery wall are the cardiologist’s most challenging adversary. When calcification is circumferential (surrounding more than 270 degrees of the vessel wall) or deeply embedded, a standard angioplasty balloon cannot generate enough force to fully expand the artery. The stent is deployed into a vessel that has not adequately dilated — and an under-expanded stent has dramatically higher rates of thrombosis and restenosis.
IVUS identifies calcium arc, thickness, and length with precision that angiography physically cannot match. Once the calcium is characterised, the cardiologist can select the appropriate modification strategy — Rotational Atherectomy (Rotablation) or Orbital Atherectomy — before the stent is placed.
Lesions longer than 25–30mm require multiple stents or very long single stents. The margin for sizing error increases with every millimetre. IVUS-guided measurement of true vessel diameter at each reference segment ensures stents are correctly sized across the entire treated length — preventing the edge mismatches that cause focal restenosis at stent margins.
The left main coronary artery supplies a majority of the heart muscle. Decisions about treating left main blockages — whether by angioplasty or bypass surgery — are among the most consequential in cardiology. Intravascular imaging is mandated by ACC/AHA guidelines for left main assessment precisely because the stakes of a misjudgement are so high. At Good Heart Clinic, no left main intervention proceeds without OCT or IVUS confirmation of lesion severity and stent result.
Where an artery branches — the main vessel and its side branch — plaque distribution is three-dimensional and cannot be captured by a flat angiographic silhouette. Intravascular imaging allows the cardiologist to see exactly how plaque is distributed around the bifurcation, choose the correct stenting strategy, and confirm that the side branch ostium (opening) remains uncompromised after the main vessel stent is deployed.
When a patient returns with recurrent symptoms after a prior angioplasty, OCT reveals whether the problem is in-stent restenosis (tissue growing back inside the stent), stent fracture, neoatherosclerosis (new plaque forming within the stent), or simple stent malapposition that was missed the first time. Each of these requires a different treatment — and none can be reliably distinguished on angiography alone.
For a thorough explanation of understanding complex coronary artery blockages — including how different lesion types are classified and what they mean for your treatment pathway — our patient education library is the clearest starting point.
OCT gives cardiologists a real-time, microscopic view inside your coronary artery — a level of detail that transforms treatment from estimation into engineering.
Optical Coherence Tomography works by emitting near-infrared light pulses from a fibre-optic probe mounted on a catheter. As the catheter is slowly withdrawn through the artery at a controlled speed, it captures cross-sectional images every fraction of a millimetre — generating a three-dimensional reconstruction of the entire treated segment with resolution approximately 10–15 microns. For reference, a human hair is approximately 70 microns wide.
Plaque composition in real time. OCT differentiates between lipid-rich plaques (soft, with a bright border and dark interior), fibrous plaques (uniform, bright), and calcified plaques (bright surface with signal drop-off behind). This differentiation determines not just whether a blockage needs treatment, but how it should be treated.
Thin-cap fibroatheroma — the rupture-prone plaque. This is the plaque type responsible for most sudden heart attacks in patients with no prior warning. It has a large lipid pool covered by an extremely thin fibrous cap — often less than 65 microns — that can rupture under mechanical stress, releasing thrombogenic material into the bloodstream and causing sudden occlusion. OCT is the only widely available technology that can reliably identify this plaque type in vivo. Identifying it allows for targeted aggressive medical therapy — or prophylactic treatment — before the rupture occurs.
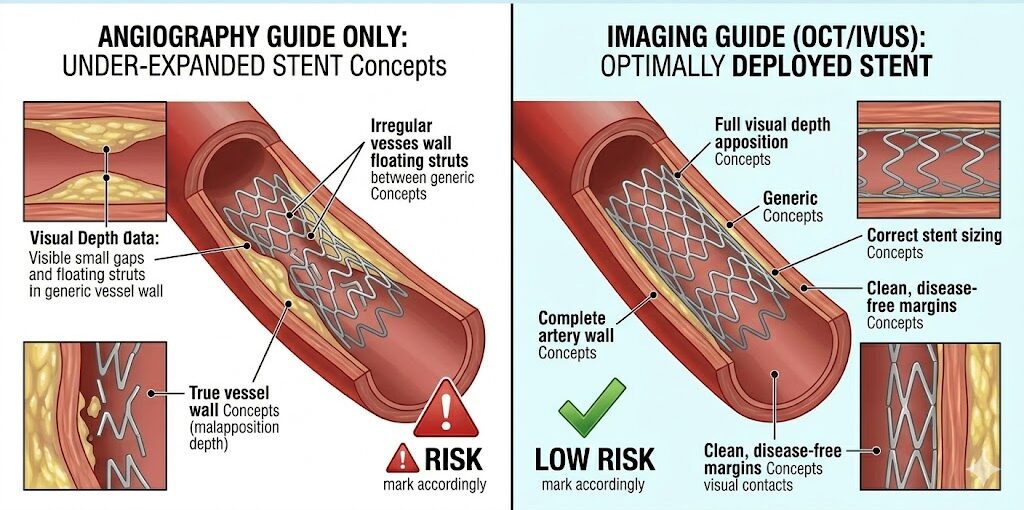
Stent strut apposition post-deployment. After a stent is placed, OCT immediately shows whether every strut is in full contact with the artery wall. Malapposed struts — those floating in the lumen — create turbulent flow and are a recognised risk factor for late stent thrombosis. OCT identifies them; the cardiologist corrects them with post-dilation before leaving the table.
Edge dissections. Small tears at the stent margins — often the entry point for restenosis — are invisible on angiography and clearly visible on OCT. If detected, they are managed immediately with stent extension.
According to a landmark study published in the AHA Journals on intravascular imaging and outcomes, OCT-guided coronary intervention is associated with significantly lower rates of major adverse cardiac events at one year compared to angiography-guided procedures — driven primarily by reductions in stent thrombosis and target vessel revascularisation.
Explore the full range of intravascular imaging procedures at Good Heart Clinic — including case examples and the clinical criteria used to select between IVUS and OCT for individual patients.
Yes — and the evidence is not marginal. Imaging-guided coronary angioplasty in Pune consistently outperforms angiography-guided procedures on every long-term outcome measure that matters to patients.
This is the question that links clinical science to patient reality. Because what patients care about — rightly — is not which imaging modality was used in the catheterisation laboratory. What they care about is: will I need to come back? Will my stent last? Can I actually live normally after this?
The answer to all three questions is meaningfully better when intravascular imaging guides the procedure.
In-stent restenosis — the re-narrowing of a stented artery due to scar tissue formation — occurs in approximately 8–15% of drug-eluting stent procedures guided by angiography alone at one year. With IVUS-guided stenting, multiple randomised controlled trials show this rate falls to 4–7%. With OCT guidance in complex lesions, rates in experienced centres fall further.
Stent thrombosis — the sudden clotting of a stent that causes a major heart attack — has a one-year incidence of approximately 0.5–1% with standard angiography guidance. With imaging-guided stenting confirming full apposition and absence of edge dissection, this rate is consistently lower across large registry data.
The mechanism is straightforward. Imaging-guided procedures produce stents that are:
Each of these factors independently reduces restenosis and thrombosis risk. Together, they substantially change the probability that a patient returns to the catheterisation laboratory within three years.
For complex lesions, Dr. Harshal Ingle routinely combines modalities — using IVUS to characterise calcium and plan the intervention, Rotablation or Orbital Atherectomy to modify the plaque where indicated, and OCT post-stenting to confirm the result. This is not a standard approach at most interventional centres in India. It is the standard at Good Heart Clinic — because the evidence supporting it is unambiguous and the patient benefit is real and measurable.
Choosing where your coronary artery is treated is not a passive decision. The cardiologist’s technical capability, the imaging technology available, and — critically — whether that cardiologist will use it when the case is complex, all determine what your life looks like three years from now.
Dr. Harshal Ingle — MD (Medicine), DrNB Cardiology, Interventional Cardiologist at Ruby Hall Clinic, Pune — is among the most technically advanced interventional cardiologists practising in Maharashtra today. His approach to complex coronary disease is built on a single principle: measure, confirm, then treat.
First in Pune — Orbital Atherectomy. When standard Rotablation reaches its anatomical limits, Orbital Atherectomy — which uses an eccentrically rotating diamond-coated crown — provides circumferential calcium modification with a single device. Dr. Ingle introduced this technique to Pune, expanding the range of calcified lesions treatable without bypass surgery.
First in Pune — Renal Denervation. A marker of catheter-based technical precision applied beyond coronary arteries — demonstrating the breadth of Dr. Ingle’s interventional skill set.
India Live 2024 presenter. Peer-reviewed case presentations at India’s leading interventional cardiology forum — reflecting a cardiologist whose work is recognised and scrutinised by the national cardiology community.
Excellence in Healthcare Award 2025 in Cardiology — presented by Maharashtra’s Health Minister and the Chief Cardiologist of Ruby Hall Clinic.
No compromise on imaging for complex cases. When a case is complex, imaging is not offered as an upgrade — it is part of the procedure. Patients at Good Heart Clinic are not asked to pay extra to have their stent placed correctly. Precision is the default.
Clinic credentials:
| Procedure | Approximate Cost (INR) |
|---|---|
| Diagnostic Coronary Angiography | ₹15,000 – ₹30,000 |
| IVUS (per vessel) | ₹25,000 – ₹45,000 |
| OCT (per vessel) | ₹35,000 – ₹60,000 |
| Rotational Atherectomy (Rotablation) + Stenting | ₹2,00,000 – ₹3,50,000 |
| Orbital Atherectomy + OCT + Stenting | ₹2,50,000 – ₹4,50,000 |
| Complex Bifurcation Angioplasty with Imaging | ₹2,00,000 – ₹4,00,000 |
| Left Main Angioplasty with IVUS/OCT | ₹2,50,000 – ₹5,00,000 |
What drives cost variation:
Insurance: Complex angioplasty procedures including atherectomy are covered under most comprehensive mediclaim and corporate health policies. Individual imaging components may have variable coverage. Our team assists proactively with pre-authorisation to avoid day-of surprises.
Rotablation (Rotational Atherectomy) uses a diamond-tipped burr spinning at up to 180,000 RPM to pulverise heavily calcified coronary plaque. It is needed when calcium is so dense or circumferential that a standard angioplasty balloon cannot cross the lesion or generate enough force to adequately expand it before stenting.
Yes. While both modify calcified plaque, Orbital Atherectomy uses an eccentrically rotating diamond-coated crown that modifies calcium in a larger, more circumferential arc with a single device size. It offers advantages in specific calcification patterns and is available at Good Heart Clinic — where Dr. Ingle performed the first case in Pune.
A regular angiogram shows the artery from outside as a 2D silhouette on X-ray — it images the blood channel, not the wall. Intravascular imaging (IVUS or OCT) travels inside the artery and captures detailed cross-sectional images of the actual wall — showing plaque composition, vessel diameter, and stent result with precision angiography cannot achieve.
No. The imaging catheter is delivered through the same sheath used for angioplasty, under local anaesthesia. Patients feel no additional discomfort from the imaging catheter itself. A brief flush of saline or contrast may cause a transient warm sensation during OCT pullback — lasting only seconds.
In many cases, yes — when advanced intravascular treatment including atherectomy and imaging-guided stenting is available. Lesions previously referred for bypass surgery are now successfully treated percutaneously at Good Heart Clinic using Rotablation or Orbital Atherectomy combined with OCT confirmation. Each case is assessed individually.
OCT confirms after stenting that the stent is fully expanded, all struts are apposed to the artery wall, and there are no edge dissections. Correcting any of these findings immediately — before the procedure ends — dramatically reduces the rates of in-stent restenosis and stent thrombosis that would otherwise lead to a repeat angioplasty.
Thin-cap fibroatheroma is a type of coronary plaque with a large lipid core covered by an extremely thin fibrous cap — under 65 microns. It is the most rupture-prone plaque type and responsible for a high proportion of sudden heart attacks. OCT is the only widely available tool that can identify it in living patients, enabling targeted treatment before rupture occurs.
Yes. Good Heart Clinic operates at Ruby Hall Clinic, Pune, where Dr. Harshal Ingle performs the full spectrum of advanced intravascular procedures — including IVUS, OCT, Rotablation, Orbital Atherectomy, and complex bifurcation and left main angioplasty — with the complete tertiary care infrastructure of Ruby Hall supporting every case.
Rotational Atherectomy (Rotablation) combined with stenting in Pune costs approximately ₹2,00,000 to ₹3,50,000 depending on the number of vessels, stent type, and imaging used. Most comprehensive mediclaim and corporate health insurance policies cover this procedure. Pre-authorisation support is provided at Good Heart Clinic.
Your cardiologist will assess your angiogram for lesion length, calcification, vessel location, and prior stent history. Signs that advanced treatment may be needed include: heavy calcification visible on angiography, prior stent with recurrent symptoms, left main involvement, or a bifurcation lesion. At Good Heart Clinic, this assessment includes intravascular imaging whenever the angiogram raises any of these concerns.
The technology exists to treat your coronary artery with the precision of engineering — to see inside it, measure it exactly, prepare it correctly, and confirm the result before the procedure ends.
Not every centre uses it. Not every cardiologist insists on it. But every patient who sits in a catheterisation laboratory with a complex coronary blockage deserves a cardiologist who will.
Intravascular treatments in Pune at Good Heart Clinic represent the current frontier of coronary intervention — not a future promise, but a present reality that your family can access today.
If you or someone you love has been told their blockage is complex, calcified, or previously stented — bring that report to Dr. Harshal Ingle. The conversation you have in that consultation may determine whether you come back in two years, or whether you simply live your life.
Book your consultation. Your heart is worth the precision.
Morning OPD — Cardiac OPD C7, Ground Floor, Building 3, Ruby Hall Clinic, Pune 411001 Evening OPD — 303A, Choice Apartments, Opp. Vohuman Cafe, Dhole Patil Road, Pune 411001 Appointments: 9822055445 / 8208950831 Cardiac Emergency: 9697020666 / 7722031119 goodheartclinic.com
OPD Timings: Monday to Saturday | Morning: 10 AM – 4 PM | Evening: 4 PM – 8 PM
We believe that every patient deserves absolute confidence in their care plan.
303, A, Choice Apartments Opp Vohuman Cafe , Dhole Patil Road , Pune
Support mail: drharshalingle@gmail.com
Opening Hours: Mon -Sat: 04.00 PM to 08.00 PM