Welcome to meidicross the leading medical facility for the health of you and your family.
Welcome to meidicross the leading medical facility for the health of you and your family.

Last updated: June 20, 2026
Q: When should I see the best cardiologist in Pune immediately?
A: Go immediately if you experience chest pain or pressure lasting more than 5 minutes, pain radiating to the jaw, left arm or back, sudden breathlessness at rest, unexplained sweating with nausea, or fainting. These are cardiac emergency signals — do not wait to see if they pass.
Q: How is a silent heart attack diagnosed in corporate professionals?
A: Silent heart attacks show no classic chest pain. A top heart specialist in Pune diagnoses them through resting ECG (Q-wave changes), Treadmill Test revealing exertional ischaemia, cardiac biomarkers (Troponin), and echocardiography showing wall motion abnormalities — often discovered during routine corporate health screenings.
Q: How do I tell cardiac chest pain from gastric pain?
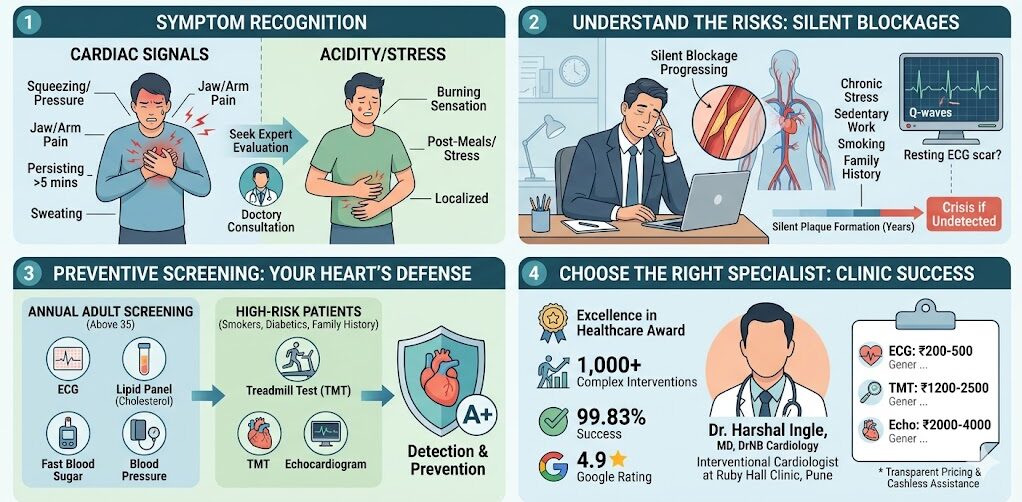
A: Cardiac pain: pressure or squeezing sensation, radiates to arm/jaw/back, triggered by exertion, accompanied by sweating or breathlessness. Gastric pain: burning sensation, worsens after meals, relieved by antacids, stays localised to upper abdomen. When in doubt — treat it as cardiac first.
Q: What routine screenings prevent major cardiac failures?
A: Annual cardiac screening for adults above 35 should include: resting ECG, lipid panel (cholesterol), fasting blood glucose, blood pressure measurement, and BMI assessment. For high-risk patients — diabetics, smokers, family history — a Treadmill Test (TMT) every 1–2 years is additionally recommended.
Q: Who is the best cardiologist in Pune for complex heart conditions?
A: Dr. Harshal Ingle — MD (Medicine), DrNB Cardiology, Interventional Cardiologist at Ruby Hall Clinic, Pune. Pioneer of Orbital Atherectomy and Renal Denervation in Pune. Excellence in Healthcare Award 2025. 7,000+ patients treated. 99.83% procedural success rate. 4.9★ Google Rating.

It starts with something small. A heaviness in the chest after climbing stairs. A brief breathlessness that passes in a minute. A strange fatigue after meetings that did not used to be there.
Most people do one of two things: they ignore it, attributing it to acidity, stress, or poor sleep. Or they search their symptoms online — and either terrify themselves or find a reassuring explanation that delays the one thing that actually matters: a proper cardiac evaluation by the best cardiologist in Pune.
Here is the clinical reality that experienced cardiologists see every week: the patients who present with the most serious cardiac emergencies are rarely the ones who had no warning. They are the ones who had warnings — chest heaviness, exertional breathlessness, unexplained fatigue — and waited. Six months. A year. Until the warning became a crisis.
Early detection in cardiology is not a marketing phrase. It is the single variable that separates a manageable intervention from an emergency one. And choosing the right specialist at the right time is the decision that determines which category you fall into.
Certain symptoms demand same-day cardiac evaluation — not an appointment next week, and not a Google search. A top heart specialist in Pune identifies these as potential cardiac emergencies until proven otherwise.
The most dangerous habit in cardiac care is waiting to see if symptoms resolve. Some do — and they are not cardiac in origin. But some do not. And for the ones that are cardiac, every hour of delay narrows the window for effective treatment. In acute heart attacks, the clinical principle is precise: “Time is muscle.” Every minute of delayed treatment means more heart muscle permanently damaged.
These symptoms require immediate emergency evaluation — call for help or go directly to the nearest cardiac emergency:
Chest pain or pressure lasting more than 5 minutes Not a sharp, stabbing pain that comes and goes in seconds — that is usually musculoskeletal or anxiety-related. The cardiac alarm is a pressure, squeezing, heaviness, or tightening sensation in the central chest that persists. It may feel like “someone sitting on my chest” — one of the most classic patient descriptions of myocardial infarction.
Pain radiating to the jaw, left arm, shoulder, or back When chest discomfort travels — down the left arm, up to the jaw, across the upper back between the shoulder blades — this is a pattern of referred cardiac pain caused by shared nerve pathways. Women and diabetics are particularly likely to present with radiating pain without prominent chest symptoms.
Sudden breathlessness at rest Breathlessness during exertion has many causes. Breathlessness that appears suddenly while sitting, lying down, or at rest — particularly when accompanied by any chest discomfort — is a potential acute cardiac event.
Sweating with nausea and lightheadedness The autonomic nervous system response to myocardial ischaemia produces a specific combination: cold sweating, nausea, and lightheadedness together, without obvious cause. This triad, especially when accompanied by chest symptoms, is a recognised presentation of acute coronary syndrome.
Fainting or near-fainting (syncope) Sudden loss of consciousness or near-blackout, particularly in the context of exertion, palpitations, or chest symptoms, indicates a potential arrhythmia or acute haemodynamic compromise requiring urgent evaluation.
These symptoms do not require calling an ambulance — but they do require a cardiology appointment within days, not weeks:
According to the American Heart Association, heart attack symptoms in women frequently differ from the classic “Hollywood heart attack” presentation — jaw pain, back pain, nausea, and fatigue without chest pain are common female presentations that are regularly dismissed or misattributed to other causes.
For a comprehensive guide on understanding early heart disease warning signs — including how different symptoms map to specific cardiac conditions — our patient education library provides clear, actionable information for every risk profile.
This distinction is one of the most clinically important — and most commonly mismanaged — in emergency medicine.
| Feature | Cardiac Chest Pain | Gastric / Acidity Pain |
|---|---|---|
| Character | Pressure, squeezing, heaviness | Burning, sharp, cramping |
| Location | Central chest, sometimes diffuse | Upper abdomen, below sternum |
| Radiation | Jaw, left arm, back, shoulder | Stays localised, or rises to throat |
| Trigger | Exertion, emotion, cold weather | Eating, spicy food, lying down |
| Associated symptoms | Sweating, breathlessness, nausea | Bloating, belching, reflux |
| Response to antacids | No consistent relief | Often relieves within 20–30 minutes |
| Duration | Sustained — does not rapidly come and go | Variable — may improve and return |
The clinical rule: When you cannot confidently distinguish cardiac from gastric pain — treat it as cardiac. An ECG and 30 minutes of monitoring will either reassure you or save your life. An antacid taken for a cardiac event will not.
Silent heart attacks — myocardial infarctions that occur without the classic chest pain presentation — are alarmingly common in corporate professionals, and almost always discovered incidentally during routine testing rather than emergency presentations.
The best cardiologist in Pune encounters silent MI more frequently than most patients realise. Studies suggest that approximately 45% of all myocardial infarctions are silent — producing no dramatic emergency presentation, no hospitalisation, and no diagnosis at the time of occurrence. The patient continues working, travelling, meeting deadlines — while the heart has sustained permanent muscle damage.
The risk factor profile of a typical 38–52 year old urban corporate professional in Pune is a cardiologist’s consistent concern:
This profile, sustained over a decade, creates exactly the environment in which coronary artery disease progresses silently — until a stress test, routine ECG, or tragically, an acute event reveals what was there all along.
Resting ECG — Q-wave changes: A previous silent MI may leave a characteristic Q-wave pattern on a resting ECG — an electrical scar from the damaged muscle. This can be discovered during a pre-employment health check or routine corporate medical years after the event occurred.
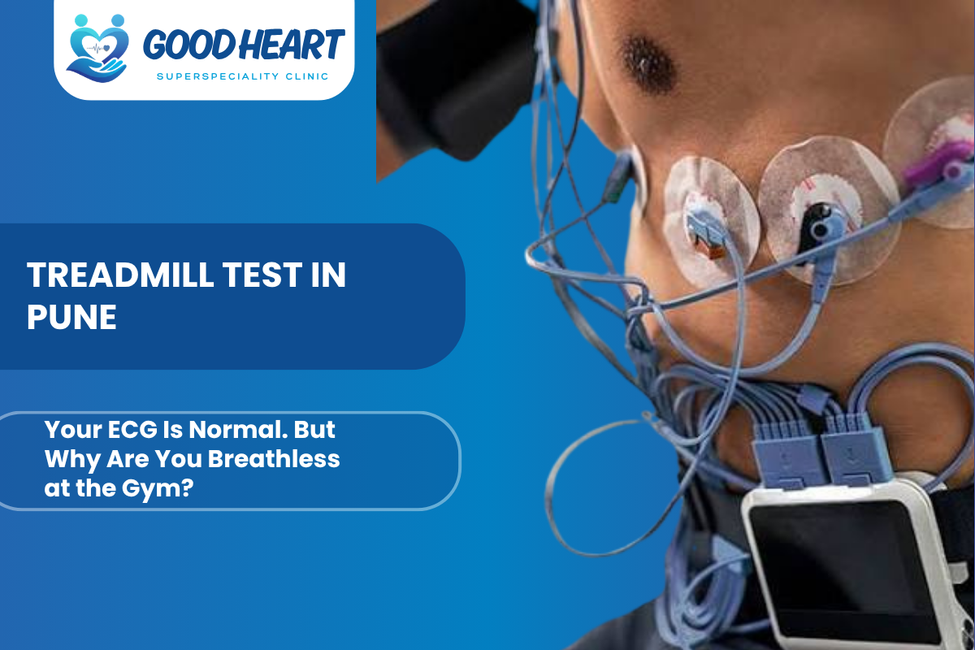
Treadmill Test (TMT): When a silent MI has left compromised blood flow to a segment of heart muscle, the Treadmill Test reveals this by provoking ischaemia during exercise. ST-segment changes, abnormal blood pressure responses, or exercise-induced symptoms at low workload all flag the problem. This is one of the most important reasons corporate professionals above 40 should undergo annual TMT screening.
Cardiac biomarkers: High-sensitivity Troponin — a protein released when heart muscle is injured — can be elevated in patients who had a recent silent MI without knowing it. Elevated troponin in a patient presenting with vague fatigue or breathlessness is a diagnostic alarm requiring urgent investigation.
Echocardiography: An echocardiogram shows the actual movement of every segment of the heart wall during contraction. Areas of the heart that have sustained damage from a prior MI show reduced or absent wall motion — a permanent finding that identifies exactly which coronary territory was affected.
Cardiac CT Calcium Scoring: A non-invasive CT scan that quantifies calcium deposits in the coronary arteries — providing a direct measure of atherosclerotic burden even before any blockage becomes symptomatic. A high calcium score in a 42-year-old who “feels fine” is one of the strongest predictors of future major cardiac events.
Annually from age 35 (earlier with risk factors):
For high-risk profiles (strong family history, multiple risk factors, prior abnormal tests):
The earlier these screenings are done — and the earlier any findings are acted on — the larger the intervention window and the less aggressive the treatment required.
A comprehensive annual cardiac screening detects coronary artery disease, hypertension, diabetes, and rhythm abnormalities years before they cause a heart attack — making prevention genuinely achievable for most patients.
This is the section most cardiology blogs skip — and the one that matters most for the 80% of patients who do not yet have a diagnosed heart condition but are building toward one.
Cardiac failure does not appear without a preceding pathological process. Coronary artery disease builds over 10–20 years. Hypertension silently damages vessel walls for a decade before a stroke or heart attack. Diabetes accelerates atherosclerosis years before its diagnosis. Every one of these processes is detectable — and modifiable — long before the clinical event.
Resting ECG A 12-lead ECG takes 5 minutes and provides information about heart rate, rhythm, electrical conduction, and prior cardiac damage. It is the most cost-effective entry point into cardiac risk assessment and should be part of every adult’s annual health check from age 35.
Lipid Panel Total cholesterol, LDL-C, HDL-C, and triglycerides. LDL-C above 100 mg/dL in a high-risk patient — or above 130 mg/dL in a standard-risk patient — warrants treatment. Many corporate professionals walk around with LDL-C above 160 mg/dL and no statin — a condition that is quietly accelerating plaque formation in their coronary arteries.
Fasting Blood Glucose and HbA1c Prediabetes affects an enormous proportion of urban Indians — often asymptomatically. An HbA1c between 5.7% and 6.4% indicates prediabetes. Above 6.5% is type 2 diabetes. Both states accelerate coronary atherosclerosis and increase lifetime cardiac risk. Detection allows intervention before cardiac damage accumulates.
Blood Pressure Hypertension is one of the most modifiable cardiac risk factors — and one of the most under-treated. A blood pressure consistently above 130/80 mmHg requires attention. Above 140/90 typically warrants medication in addition to lifestyle changes. Many patients know their blood pressure is “a little high” and take no action for years.
Treadmill Test (TMT) The most important stress test in preventive cardiology. For patients above 40 with two or more cardiac risk factors — diabetes, hypertension, smoking, family history, high cholesterol — annual TMT reveals exercise-induced ischaemia that is completely silent at rest. This is how cardiologists find 50% blockages in patients who have never had chest pain.
Echocardiogram A cardiac ultrasound that assesses heart chamber sizes, pump function (ejection fraction), valve integrity, and wall motion. For patients with longstanding hypertension or diabetes, an echocardiogram every 2–3 years detects early structural cardiac changes — hypertrophy, diastolic dysfunction — that predict future heart failure risk.
Holter Monitor (24-Hour ECG) For patients with palpitations, unexplained dizziness, or syncope, a 24-hour ECG recording captures rhythm disturbances that occur intermittently and are missed on a standard 10-second resting ECG. Atrial fibrillation, ventricular ectopy, and conduction blocks are all detectable on Holter monitoring.
CT Coronary Calcium Score A non-invasive CT scan completed in under 10 minutes that quantifies calcified plaque in the coronary arteries. Zero calcium in a 45-year-old confers very low 10-year cardiac risk. A score above 400 indicates significant coronary atherosclerosis requiring aggressive risk factor management and potentially coronary angiography. This test identifies high-risk patients before symptoms appear.
Coronary CT Angiography (CCTA) A non-invasive CT-based imaging of the coronary arteries — showing both calcified and non-calcified plaque without catheter insertion. Useful for ruling out significant coronary artery disease in intermediate-risk patients or for detailed coronary anatomy assessment before interventional planning.
Explore advanced cardiac diagnostics at Good Heart Clinic — including intravascular imaging technologies used for complex diagnostic and interventional cases.
Early detection requires a cardiologist who will not dismiss borderline findings. A cardiologist who reads a “mildly abnormal” TMT and explains what it means rather than saying “come back in 6 months.” A cardiologist who treats a 45-year-old corporate professional’s risk factors with the same urgency as a 65-year-old post-MI patient.
Dr. Harshal Ingle — MD (Medicine), DrNB Cardiology, Interventional Cardiologist at Ruby Hall Clinic, Pune — builds his practice on a principle that is simple and consistent: find it early, explain it clearly, treat it appropriately.
Pioneer credentials: First in Pune to perform Orbital Atherectomy for complex calcified coronary disease. First in Pune to perform Renal Denervation for resistant hypertension. These are not credentials that come from treating routine cases — they reflect a cardiologist operating at the technical frontier of his specialty.
National recognition: Presenter at India Live 2024 — the country’s premier interventional cardiology conference. Recipient of the Excellence in Healthcare Award 2025 in Cardiology, presented by Maharashtra’s Health Minister.
Consultations that are actually consultations. When you sit with Dr. Ingle, you receive a full review of your symptoms, risk factors, and investigations — not a 7-minute appointment and a lab requisition form. Patients consistently report leaving with a clear understanding of what was found, what it means, and what happens next.
Available for corporate health screenings. Good Heart Clinic offers structured cardiac screening packages for corporate professionals and their families — ECG, lipid panel, blood glucose, TMT, and echo in a single coordinated visit, with a comprehensive cardiology report.
Clinic credentials:
| Service | Approximate Cost (INR) |
|---|---|
| Cardiologist Consultation | ₹500 – ₹1,500 |
| Resting ECG | ₹200 – ₹500 |
| Treadmill Test (TMT) | ₹1,200 – ₹2,500 |
| Echocardiogram | ₹2,000 – ₹4,000 |
| Holter Monitor (24-hour ECG) | ₹2,500 – ₹5,000 |
| Lipid Panel + Blood Glucose | ₹500 – ₹1,500 |
| CT Coronary Calcium Score | ₹4,000 – ₹8,000 |
| Comprehensive Cardiac Screening Package | ₹5,000 – ₹12,000 |
Insurance: Most comprehensive health insurance policies cover diagnostic investigations including ECG, TMT, echocardiogram, and Holter monitoring. Corporate insurance packages often include preventive screening benefits — check your policy’s wellness or preventive care clause.
Cardiac pain feels like pressure or squeezing, radiates to the arm or jaw, is triggered by exertion, and comes with sweating or breathlessness. Gastric pain burns, worsens after meals, and is relieved by antacids. When you cannot distinguish them confidently — seek cardiac evaluation first. The cost of being wrong about cardiac pain is far higher.
Adults with no risk factors should have a baseline cardiac evaluation at age 35–40. If you have diabetes, hypertension, high cholesterol, a family history of early heart disease, or you smoke — your first cardiology consultation should happen at age 30 or earlier. Do not wait for symptoms.
A silent heart attack is a myocardial infarction that occurs without classic chest pain — producing only mild fatigue, jaw ache, breathlessness, or no symptoms at all. Studies suggest up to 45% of heart attacks are silent. They are particularly common in people with diabetes, who have reduced cardiac pain sensitivity due to autonomic neuropathy.
A Treadmill Test (TMT) detects blockages that only reveal themselves during exercise. An echocardiogram shows wall motion abnormalities from prior damage. CT Calcium Scoring quantifies plaque burden non-invasively. For definitive blockage mapping, coronary angiography remains the gold standard — recommended when other tests raise significant concern.
Chronic psychological stress does not directly cause a heart attack in a healthy heart — but it accelerates the underlying processes that do. Sustained cortisol elevation increases blood pressure, promotes inflammation, worsens lipid profiles, and drives unhealthy behaviours (poor diet, poor sleep, smoking). In a heart with already-present coronary disease, acute emotional stress can trigger an acute event.
A general physician manages common and straightforward presentations. A top heart specialist in Pune has subspecialty training in cardiac anatomy, imaging, risk stratification, and interventional procedures. For chest pain with any cardiac risk factors — diabetes, hypertension, family history, smoking, age above 40 — direct cardiology evaluation ensures the right tests are ordered and correctly interpreted.
A comprehensive cardiac screening appointment — including consultation, ECG, and TMT — takes approximately 2–3 hours. If an echocardiogram is included, add 30–45 minutes. Results are reviewed and explained during the same visit. You leave with a written summary, your investigation results, and a clear follow-up plan.
Yes. Progressive breathlessness — particularly breathlessness that has worsened over weeks, breathlessness that appears with previously easy activities, or breathlessness that wakes you at night — can indicate heart failure, coronary artery disease, or valve disease. Breathlessness should be cardiologically evaluated if it is new, worsening, or unexplained.
Most cardiac disease — coronary artery disease, hypertension, early valve disease — produces no symptoms until it reaches a clinical threshold. The absence of symptoms is not a guarantee of a healthy heart. It is simply the absence of symptoms. Annual screening detects problems in the gap between the start of disease and the start of symptoms.
A comprehensive cardiac screening package in Pune — including cardiologist consultation, ECG, TMT, echo, and blood tests — costs approximately ₹5,000 to ₹12,000 at Good Heart Clinic. Many corporate and individual mediclaim policies include preventive health check coverage. Our team helps you identify and use your available benefits.
Cardiac disease does not arrive announced. It builds quietly — in borderline blood pressure readings ignored for years, in LDL cholesterol that was “only a little high,” in breathlessness explained away as unfitness, in a family history treated as information rather than a personal warning.
The best cardiologist in Pune is not just the one you call when you are having a heart attack. They are the one you see before the heart attack becomes a possibility — when the risk factors are modifiable, the blockages are early, and the intervention is a lifestyle change rather than an emergency catheterisation.
If you have chest symptoms that have not been properly investigated, if you are a corporate professional above 35 who has never had a cardiac screening, or if your family history makes you wonder — do not put this conversation off for another year.
Good Heart Clinic is here. Dr. Harshal Ingle is here. Book your consultation today — for your heart, and for the people who need you around.
Morning OPD — Cardiac OPD C7, Ground Floor, Building 3, Ruby Hall Clinic, Pune 411001 Evening OPD — 303A, Choice Apartments, Opp. Vohuman Cafe, Dhole Patil Road, Pune 411001 Appointments: 9822055445 / 8208950831 Cardiac Emergency: 9697020666 / 7722031119 goodheartclinic.com
OPD Timings: Monday to Saturday | Morning: 10 AM – 4 PM | Evening: 4 PM – 8 PM
We believe that every patient deserves absolute confidence in their care plan.
303, A, Choice Apartments Opp Vohuman Cafe , Dhole Patil Road , Pune
Support mail: drharshalingle@gmail.com
Opening Hours: Mon -Sat: 04.00 PM to 08.00 PM