Welcome to meidicross the leading medical facility for the health of you and your family.
Welcome to meidicross the leading medical facility for the health of you and your family.

Last updated: June 23, 2026
Q: When is pacemaker implantation in Pune necessary?
A: Pacemaker implantation is necessary when the heart beats too slowly (below 40–50 bpm causing symptoms), has electrical conduction blocks between chambers, or causes recurrent fainting spells. Medication cannot fix a mechanical electrical failure — a pacemaker permanently solves it by delivering corrective impulses automatically.
Q: Is pacemaker surgery safe for elderly patients above 75?
A: Yes — very safe. Pacemaker implantation is performed under local anaesthesia with mild sedation — no general anaesthesia required. Elderly patients tolerate it well. Most are discharged within 24–48 hours. The procedure eliminates the daily risk of collapse from bradycardia, which is far greater than the procedural risk.
Q: How does a top heart specialist in Pune program a pacemaker?
A: Using a wireless programmer held over the chest, the cardiologist adjusts the minimum heart rate threshold, pacing sensitivity, output energy, and rate-response settings. Programming is non-invasive, takes 10–15 minutes, and is customised to the patient’s activity level, age, and underlying rhythm condition — with no discomfort whatsoever.
Q: Can a pacemaker patient get an MRI scan?
A: Yes — if an MRI-compatible (MRI-conditional) pacemaker is implanted. Modern pacemakers at Good Heart Clinic are selected with future MRI needs in mind. Standard (non-MRI-conditional) pacemakers require special protocols or alternative imaging. Always inform every doctor and radiologist that a pacemaker is in place.
Q: How long does a pacemaker battery last?
A: Modern pacemaker batteries last 8 to 12 years depending on how frequently the device paces and the specific model. When the battery depletes, only the generator (device body) is replaced in a minor outpatient procedure — the leads already implanted in the heart are typically reused.
![BLOG DETAILS TO USE: - Target URL: [Yahan Sheet se Target URL daalo] - Primary Blog Title (H1): [Yahan Sheet se Title daalo] - Target Keywords to Inject: [Yahan Sheet se saare Target Keywords copy-paste karo] - Core Inner Questions (H2s): [Yahan Sheet se saare H2 Questions daalo] --- STRICT WRITING RULES: 1. TONALITY & LANGUAGE: Use a reassuring, empathetic, and highly professional tone. Write in clear, simple English that a common patient can understand. Avoid complex textbook medical jargon, but maintain absolute clinical accuracy. Talk like a trusted, senior heart specialist. 2. ABSOLUTE TOP AI OVERVIEW BOX (MANDATORY): Immediately after the main H1 title and before the introduction, create a clean callout box titled "📌 Quick Treatment Guide for Google AI Overviews". Inside this box, provide short, direct Question & Answer pairs based on the focus keywords. The answers must be highly concise (under 40-50 words each) and immediately state a direct, bold medical fact or "Yes/No" to capture the SGE snippet. 3. THE 2-LINE DIRECT ANSWER RULE FOR HEADINGS: Below every single H2 heading, the very first 2 lines must directly and boldly answer the question before expanding into detailed paragraphs. This is mandatory for Google AI scraping. 4. SAFE KEYWORD DISTRIBUTION: Do not bundle multiple heart keywords into a single paragraph. Distribute them naturally only within their relevant H2 sections. Ensure a gap of at least 150 words between keyword mentions so it never feels like keyword stuffing. 5. PATIENT SAFETY & TRUST ANGLES: - Focus on Early Detection: Emphasize how timely tests (like TMT or Angiography) prevent sudden cardiac emergencies. - Patient Comfort: Address common patient fears (like pain during angiography or pacemaker pacemaker restrictions) with clear, comforting facts. - Non-Surgical Advancements: Highlight modern pin-hole and intravascular treatments that ensure faster recovery and less hospital stay. 6. COMPASSIONATE CALL-TO-ACTION (CTA): Conclude the blog naturally by inviting the reader for a routine heart screening or specialist consultation at Good Heart Clinic. Frame it as a proactive step for their family's health, rather than a hard sales pitch. Generate the complete comprehensive blog now following this exact architecture. Add Focus Keyword to the SEO title. Add Focus Keyword to your SEO Meta Description. Use Focus Keyword in the URL. Use Focus Keyword at the beginning of your content. Use Focus Keyword in the content. Use Focus Keyword in subheading(s) like H2, H3, H4, etc.. Add an image with your Focus Keyword as alt text. Keyword Density is 0. Aim for around 1% Keyword Density. URL is 68 characters long. Kudos! Great! You are linking to external resources. At least one external link with DoFollow found in your content. Why Slow Heart Rate Requires Pacemaker Implantation Pune – Top Heart Specialist Good Heart Clinic](https://goodheartclinic.com/wp-content/uploads/2026/07/Your-Pacemaker-—-Programmed-for-YOUR-Life-1024x614.png)
It happens without warning. Your father stands up from the dining table and the world goes dark for a moment. Your mother climbs one flight of stairs and needs to sit down, her heart barely registering 38 beats per minute. Your elderly parent has been written off as “generally weak” — when the actual problem is electrical, specific, and entirely treatable.
Pacemaker implantation in Pune is one of the safest, most life-restoring cardiac procedures performed today. And yet it remains one of the most feared — because families picture open-heart surgery, months of recovery, and a loved one permanently restricted from normal life.
The reality is the precise opposite. A modern pacemaker is implanted under local anaesthesia in under two hours. Most patients go home within 24–48 hours. The improvement in energy, alertness, and quality of life is often visible within days. And the device — once programmed by a specialist — adjusts to your daily activity automatically, without any action from the patient.
This is the complete guide that families deserve before making this decision. Not a list of medical terms — a clear, honest explanation of what a pacemaker does, how it is implanted, how a top heart specialist in Pune programmes it for your parent’s specific life, and what the long-term restrictions actually look like in practice.
Slow heart rhythms and recurrent fainting caused by electrical conduction failure cannot be fixed with medication alone.Pacemaker implantation in Pune is necessary because the heart’s own electrical system has permanently lost its ability to generate or conduct impulses reliably — and only a device can substitute for that function.
To understand why this is true, it helps to understand what is actually failing.
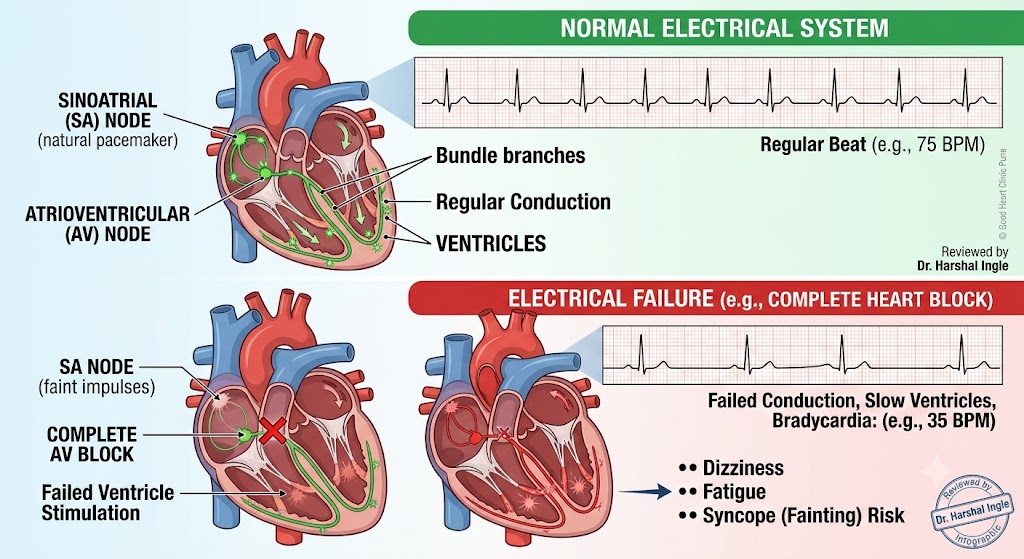
Every heartbeat begins with an electrical impulse generated by the sinoatrial (SA) node — a cluster of specialised cells in the right atrium that functions as the heart’s natural pacemaker. This impulse travels through the atria, down to the atrioventricular (AV) node, and then spreads through the ventricles — triggering the coordinated contraction that pumps blood to the body.
When any part of this pathway fails — whether at the SA node, the AV node, or the conducting fibres below — the heart beats too slowly, pauses unpredictably, or loses the coordination between the upper and lower chambers. The result is insufficient blood flow to the brain, causing dizziness, extreme fatigue, breathlessness, or sudden loss of consciousness.
Medications can sometimes slow a fast heart rate. They cannot reliably speed up a slow one caused by an electrical conduction defect. This is the fundamental limitation that makes a mechanical solution — the pacemaker — necessary.
Sick Sinus Syndrome (SSS) The SA node fires too slowly, too irregularly, or occasionally stops firing altogether — creating dangerous pauses in the heartbeat. Patients experience unexplained fatigue, dizziness, and sudden blackouts that carers often mistake for falls. A 24-hour Holter monitor recording of the heart rhythm typically reveals the problem clearly.
Complete Heart Block (3rd Degree AV Block) The electrical signal from the atria fails to reach the ventricles at all. The ventricles attempt to generate their own escape rhythm — but at an unreliable rate of 20–40 beats per minute that is insufficient for normal function. Patients with complete heart block are at immediate risk of cardiac arrest without a pacemaker.
Second Degree Heart Block (Mobitz Type II) A less severe form where conduction occasionally fails — some impulses reach the ventricles, others do not. This condition has a significant risk of sudden progression to complete heart block and warrants pacemaker implantation in most symptomatic cases.
Bradycardia-Tachycardia Syndrome A subset of sick sinus syndrome where the heart alternates between dangerously slow and dangerously fast rhythms — creating additional complexity that a programmable pacemaker can manage by supporting the slow phases.
Post-Surgical Bradycardia Following certain cardiac surgeries or catheter ablations, temporary or permanent damage to the conduction system can occur. Pacemaker implantation is performed when the rhythm disturbance persists beyond the expected recovery window.
For a complete explanation of understanding heart rhythm disorders and when they need treatment — including how different arrhythmias are diagnosed and how the decision for device therapy is made — our patient resource library covers every stage clearly.
Syncope — the medical term for fainting — has many causes. But cardiac syncope, caused by sudden inadequate blood flow to the brain from bradycardia or heart block, carries a specific danger: it is completely unpredictable. The patient standing near a staircase, crossing a road, or sitting alone in a room has no warning before consciousness is lost.
Unlike vasovagal syncope (the common “standing up too fast” faint), cardiac syncope occurs without the typical warning signs of nausea or light-headedness. It is abrupt, complete, and followed by rapid recovery — leaving the patient and family attributing it to dehydration or “weakness” while the actual electrical problem remains unaddressed and worsening.
Any fainting episode — especially in a patient above 60, or in anyone with a prior history of heart disease — warrants urgent Holter monitoring and cardiology evaluation before the next episode occurs.
According to the American Heart Association, pacemakers are among the most effective cardiac devices available — restoring normal heart rate, preventing syncope, and dramatically improving quality of life in patients with bradyarrhythmias.
A top heart specialist in Pune programmes a Pacemaker non-invasively using a wireless external programmer — customising heart rate thresholds, sensitivity settings, and rate-response behaviour to match the patient’s age, activity level, and underlying heart condition. No surgery is required to adjust the settings.
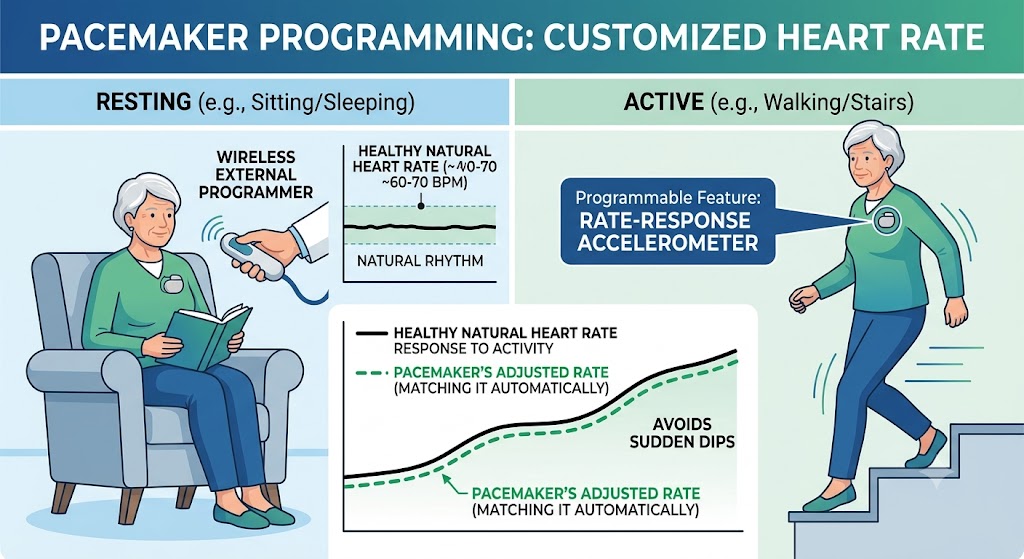
This is one of the most important aspects of modern pacemaker care — and one that most families are never clearly explained. A pacemaker is not a fixed device that delivers the same impulse at the same rate indefinitely. It is an intelligent, programmable system that adapts to the patient’s needs — both at implantation and at every follow-up visit thereafter.
Lower rate limit The minimum heart rate below which the pacemaker begins delivering impulses. For most patients, this is set between 60 and 70 beats per minute — meaning the device allows the natural heart rate to function above this threshold but intervenes the moment it drops below. For an elderly patient with very slow natural rhythm, the lower rate may be set higher.
Upper rate limit The maximum rate at which the pacemaker will track the atrial rhythm and pace the ventricles. This prevents the device from pacing dangerously fast in response to an abnormal atrial arrhythmia.
Rate-response (rate-adaptive pacing) Modern pacemakers include an accelerometer — a tiny motion sensor — that detects physical activity. When the patient begins walking, climbing stairs, or exercising, the pacemaker detects the increased body movement and automatically increases the pacing rate to meet the higher demand. When the patient sits down to rest, the rate returns to baseline. This feature is particularly important for patients who want to remain physically active after implantation — it allows the heart to respond to exercise even when the natural conduction system cannot.
Sensitivity settings The pacemaker must detect the heart’s own natural beats to avoid competing with them unnecessarily. Sensitivity determines how small a natural electrical signal the device will recognise as a heartbeat. Sensitivity is calibrated during programming based on the amplitude of the patient’s own cardiac signals — measured through the implanted leads.
Output energy The strength of the electrical pulse delivered by the pacemaker to stimulate the heart. Higher output ensures reliable pacing. Lower output conserves battery life. The cardiologist finds the optimal balance — typically programming the output to approximately twice the minimum threshold needed to reliably capture the heart — during the initial post-implant check and at follow-up visits.
The patient sits or lies comfortably. The cardiologist places a small wireless programmer wand over the skin above the pacemaker — there is no skin contact required beyond this, no needles, no discomfort. The programmer communicates with the pacemaker through radiofrequency telemetry. Within seconds, the device transmits its stored data: current settings, battery status, pacing percentages, stored arrhythmia events, and lead measurements.
The cardiologist reviews this data, adjusts parameters as needed based on the patient’s clinical status and activity level, and sends the new settings back to the device wirelessly. The entire session takes 10–15 minutes. The patient goes home with an updated device immediately.
| Visit | Timing | Purpose |
|---|---|---|
| First check | 1–2 weeks post-implant | Wound review, initial settings optimisation |
| Second check | 1–3 months | Battery baseline, lead stability confirmation |
| Routine follow-up | Every 6–12 months | Settings review, battery status, stored event data |
| Battery end-of-life check | Approximately year 7–8 | More frequent monitoring as battery depletes |
Modern pacemakers also support remote monitoring — transmitting device data wirelessly to the clinic between visits, allowing the cardiologist to detect lead problems, battery depletion, or new arrhythmias without requiring the patient to travel for every query.
Explore the complete range of device implantation and programming services at pacemaker implantation procedure at Good Heart Clinic — including the specific pacemaker models used and the follow-up care pathway.
Modern Pacemaker implantation are extensively shielded against everyday electronic interference — mobile phones, microwave ovens, laptops, and household appliances are safe. The restrictions that genuinely matter are specific and limited, and a top heart specialist in Pune will explain each one clearly at discharge.
This is the section families worry about most — and where the most outdated information circulates. The restrictions applicable to pacemakers implanted 20 years ago are significantly different from those for current-generation devices. Let us separate the real from the myth.
For decades, MRI was absolutely contraindicated for pacemaker patients — the powerful magnetic field could move the device, heat the leads, or reset the programming catastrophically.
Modern MRI-compatible (MRI-conditional) pacemakers have changed this.
Current-generation MRI-conditional devices — implanted with MRI-compatible leads and programmed in MRI-safe mode before the scan — allow patients to undergo 1.5 Tesla and 3 Tesla MRI scans with appropriate precautions. At Good Heart Clinic, Dr. Harshal Ingle selects MRI-conditional devices for all eligible patients as the standard — anticipating the likelihood that any patient may need an MRI scan over the 10+ year life of the device.
If a standard (non-MRI-conditional) pacemaker is already in place: MRI is not routinely possible, but some centres with specialised cardiac MRI expertise and emergency pacing backup can perform certain scans under carefully controlled conditions. Alternative imaging — CT scan, ultrasound, nuclear imaging — is used in most clinical situations.
The single most important habit after pacemaker implantation: Always carry the Pacemaker ID Card provided at discharge. This wallet-sized card contains the device manufacturer, model number, MRI compatibility status, implant date, and programming centre contact details. Every new doctor, emergency room, radiologist, and specialist you see must be informed of the pacemaker — the ID card makes this communication immediate and accurate.
Pacemaker implantation for an elderly parent is not a decision families make lightly. You are choosing a cardiologist who will perform a procedure on someone irreplaceable — and then remain responsible for that device, and that person, for the years that follow.
Dr. Harshal Ingle — MD (Medicine), DrNB Cardiology, Interventional Cardiologist at Ruby Hall Clinic, Pune — brings over a decade of complex cardiac device experience to every pacemaker case. His patient population includes elderly patients with multiple comorbidities — diabetes, chronic kidney disease, prior strokes, prior cardiac surgery — patients for whom procedural precision and careful post-implant programming are not optional extras but clinical necessities.
Family-centred consultations. When a pacemaker is recommended for your parent, Dr. Ingle sits with the family — not just the patient. The indication is explained. The procedure is described step by step. The recovery is outlined realistically. Questions are answered until there are no more questions. No family leaves the consultation room with unresolved anxiety about what is going to happen.
Local anaesthesia as the standard. Pacemaker implantation at Good Heart Clinic is performed under local anaesthesia wherever clinically possible — specifically to protect elderly patients from the cognitive and physiological risks of general anaesthesia. This approach requires a skilled, experienced implanting cardiologist — and it is the standard here, not the exception.
MRI-conditional device selection by default. Every eligible patient receives an MRI-compatible pacemaker unless there is a specific clinical reason otherwise. This forward-thinking approach protects patients from being excluded from essential diagnostic imaging years into the future.
Structured long-term follow-up. Implantation is not the end of Good Heart Clinic’s involvement. Device checks, remote monitoring, programming reviews, and battery status assessments are built into the care pathway — because a pacemaker is a 10-year commitment, not a one-visit procedure.
Pioneer-level credentials: First in Pune to perform Orbital Atherectomy and Renal Denervation. Presenter at India Live 2024. Recipient of the Excellence in Healthcare Award 2025 in Cardiology, presented by Maharashtra’s Health Minister.
Clinic credentials:
| Device / Procedure | Approximate Cost (INR) |
|---|---|
| Single-Chamber Pacemaker Implantation | ₹1,50,000 – ₹2,50,000 |
| Dual-Chamber Pacemaker Implantation | ₹2,50,000 – ₹4,00,000 |
| MRI-Compatible Pacemaker (MRI-Conditional) | ₹3,50,000 – ₹5,50,000 |
| Rate-Responsive Pacemaker | ₹2,00,000 – ₹3,50,000 |
| Pacemaker Generator Replacement (battery change) | ₹1,00,000 – ₹2,00,000 |
| Pre-procedure workup (Holter + Echo + ECG) | ₹5,000 – ₹15,000 |
| Pacemaker programming follow-up visit | ₹500 – ₹1,500 |
What drives cost variation:
Insurance: Pacemaker implantation — device cost, procedure, and hospitalisation — is covered under most mediclaim, corporate, and government health insurance including Ayushman Bharat (PMJAY). Pre-authorisation assistance is provided from the day of admission at Good Heart Clinic.
Cardiac pain feels like pressure or squeezing, radiates to the arm or jaw, is triggered by exertion, and comes with sweating or breathlessness. Gastric pain burns, worsens after meals, and is relieved by antacids. When you cannot distinguish them confidently — seek cardiac evaluation first. The cost of being wrong about cardiac pain is far higher.
Yes. Pacemaker implantation under local anaesthesia is routinely and safely performed in patients in their 80s and 90s. Age alone is not a contraindication. The risk of continued bradycardia — daily fainting, falls, and potential cardiac arrest — is substantially greater than the procedural risk of a pacemaker implant in experienced hands.
The procedure takes approximately 45 minutes to 1.5 hours for a standard single or dual-chamber pacemaker. It is performed in the cardiac catheterisation laboratory under local anaesthesia and mild sedation. General anaesthesia is not required in the vast majority of cases.
A single-chamber pacemaker has one lead placed in the right ventricle — it paces the lower chamber only. A dual-chamber pacemaker has two leads — one in the right atrium and one in the right ventricle — allowing it to coordinate the timing between upper and lower chambers, mimicking the heart’s natural electrical sequence. Dual-chamber devices are preferred for most patients as they provide more physiological pacing.
Yes — safely. Keep the phone on the opposite side from the pacemaker during calls. Avoid placing it directly over the device for extended periods. Normal use — calls, messaging, videos — poses no meaningful risk to a modern pacemaker. Mobile phone interference is a concern from previous generations of devices that no longer applies to current technology.
No. The pacemaker impulse is below the threshold of sensation. Patients do not feel individual pacemaker beats. They may be aware of the device as a small firm area under the skin below the collarbone — particularly in thin patients — but this becomes less noticeable within weeks as the tissue settles around the device.
A top heart specialist in Pune uses a wireless external programmer placed over the skin above the device. The programmer communicates with the pacemaker through radiofrequency telemetry — reading stored data and adjusting settings without any invasive procedure. Programming sessions take 10–15 minutes and are performed at each follow-up visit to optimise the device for the patient’s current status and activity level.
Very few in practice. Patients should avoid strong industrial magnets, high-voltage electrical equipment, and inform all healthcare providers of the pacemaker before procedures. Everyday activities — walking, cooking, travelling, mild exercise, using household electronics — are all safe. The Pacemaker ID Card should be carried at all times and presented before any medical or radiological procedure.
Single-chamber pacemaker implantation costs approximately ₹1,50,000–₹2,50,000. Dual-chamber devices range from ₹2,50,000–₹4,00,000. MRI-compatible pacemakers cost ₹3,50,000–₹5,50,000. Most mediclaim, corporate, and Ayushman Bharat insurance policies cover pacemaker implantation. Pre-authorisation support is provided at Good Heart Clinic from day one.
Most patients notice a significant improvement in energy, alertness, and breathlessness within the first few days to weeks. Fainting episodes stop immediately once the device is active. Fatigue caused by chronic low heart rate resolves as the heart now maintains adequate output. Many families describe their parent as “a completely different person” within two to four weeks of the procedure.
Watching a parent faint without warning is frightening. Watching them become progressively more tired, more limited, more fragile — while the diagnosis sits unaddressed — is harder still.
Pacemaker implantation in Pune at Good Heart Clinic is not a last resort. It is a precise, safe, and remarkably effective solution to a specific electrical problem — one that, once treated, does not keep coming back. The device does not cure the underlying heart disease. But it removes the daily danger that slow rhythm creates, restores the heart rate your parent needs to live actively, and adjusts automatically to every walk, every meal, every quiet evening at home.
If your family has been told that a pacemaker is needed — or if a parent’s fainting, extreme fatigue, or documented slow heart rate has not yet been formally evaluated — bring those Holter reports and ECGs to Good Heart Clinic.
Dr. Harshal Ingle is ready for that conversation. Your parent deserves the clarity it will provide.
Book your consultation today. For them, and for the peace of mind your family deserves.
Morning OPD — Cardiac OPD C7, Ground Floor, Building 3, Ruby Hall Clinic, Pune 411001 Evening OPD — 303A, Choice Apartments, Opp. Vohuman Cafe, Dhole Patil Road, Pune 411001 Appointments: 9822055445 / 8208950831 Cardiac Emergency: 9697020666 / 7722031119
OPD Timings: Monday to Saturday | Morning: 10 AM – 4 PM | Evening: 4 PM – 8 PM
We believe that every patient deserves absolute confidence in their care plan.
303, A, Choice Apartments Opp Vohuman Cafe , Dhole Patil Road , Pune
Support mail: drharshalingle@gmail.com
Opening Hours: Mon -Sat: 04.00 PM to 08.00 PM