Welcome to meidicross the leading medical facility for the health of you and your family.
Welcome to meidicross the leading medical facility for the health of you and your family.

Last updated: June 17, 2026
Q: Can coronary angioplasty in Pune replace bypass surgery?
A: Yes — in most cases. Coronary angioplasty restores blood flow through a pin-hole wrist procedure using a balloon and stent. For single, double, and many triple vessel blockages, it delivers outcomes equivalent to bypass surgery without open-heart operation, general anaesthesia, or weeks of recovery.
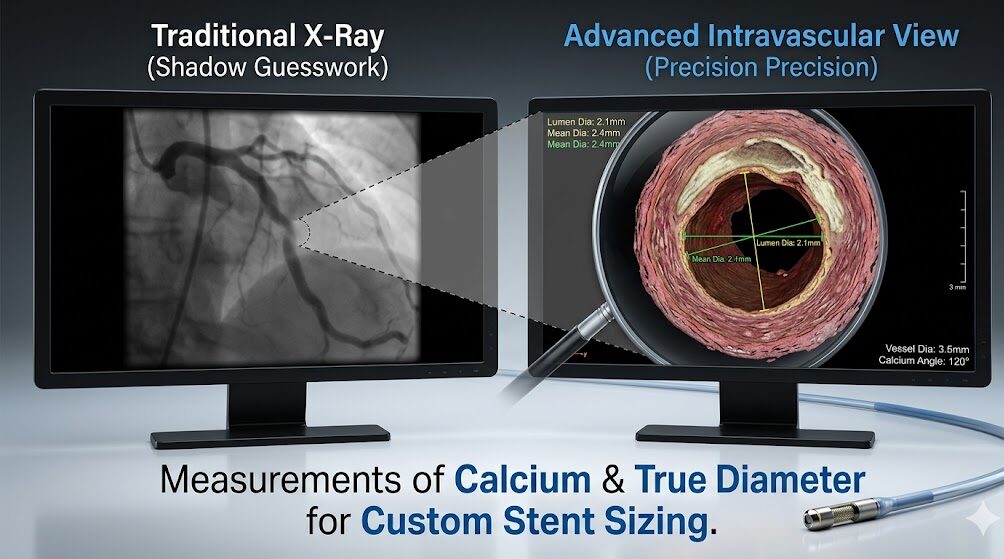
Q: Why are intravascular treatments in Pune needed for calcified blockages?
A: Heavily calcified arteries resist standard balloon expansion. IVUS and OCT imaging precisely measure calcium severity, while Rotablation or Orbital Atherectomy pulverises the calcium before stenting. Without this preparation, stents under-expand — dramatically increasing the risk of re-blockage and stent clotting.
Q: How long does a drug-eluting stent (DES) last?
A: A drug-eluting stent is permanent — it does not expire. With correct antiplatelet medication for 6–12 months and sustained lifestyle changes, DES provides durable, long-term arterial patency. Re-blockage rates are under 5–10% at one year in experienced centres using imaging-guided implantation.
Q: Is IVUS or OCT imaging necessary during angioplasty?
A: For complex, calcified, long, or bifurcation lesions — yes, strongly recommended. Intravascular imaging confirms correct stent sizing, full expansion, and absence of edge tears before the procedure ends. Studies show it reduces major cardiac events by 30–40% compared to angiography-guided stenting alone.
Q: What is the recovery time after coronary angioplasty in Pune?
A: Most patients are discharged the same day or next morning. Light activity resumes within 2–3 days. Desk work within 1–2 weeks. Full normal activity within 4–6 weeks. The wrist (radial) approach means no prolonged bed rest and no groin wound management.
“The doctor said I need a heart operation.”
That sentence lands differently when it is your own heart being discussed. Immediately, the mind fills with images from movies — an open chest, a heart-lung machine, weeks of recovery, the family’s fear in the waiting room.
But here is the clinical truth most patients are not told clearly enough: the majority of coronary artery blockages in India today do not require open-heart bypass surgery. They can be treated through a pin-hole at the wrist, using a catheter, a balloon, and a stent — with the patient awake, the procedure complete in under an hour, and discharge happening the same day or the following morning.
Coronary angioplasty in Pune has advanced to a point where even the most complex, calcified, previously considered “inoperable” blockages are now being cleared without a surgical incision — using a combination of intravascular imaging, plaque modification technology, and next-generation drug-eluting stents that perform reliably for years.
This blog explains exactly how — for the patient who has just been told they have a blocked artery and deserves to know all their options.
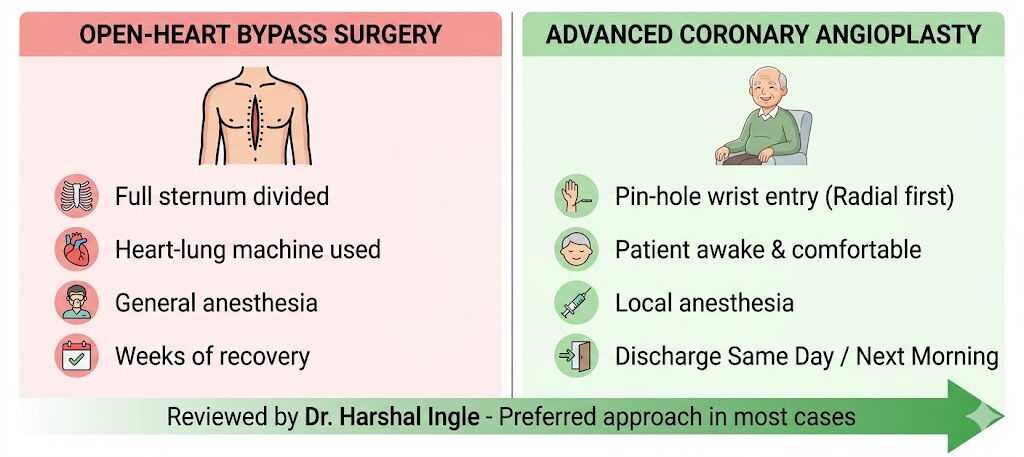
Modern coronary angioplasty in Pune restores blood flow by physically opening the blocked artery from the inside — using a catheter, a balloon, and a stent — without cutting through the chest, stopping the heart, or using a bypass machine.
This is the fundamental distinction that changes everything for patients: bypass surgery reroutes blood around the blockage by creating a new vessel pathway. Angioplasty opens the blocked vessel itself. No detour. No grafts harvested from the leg. No sternum divided. No general anaesthesia. No intensive care unit.
Access: A thin catheter sheath is introduced through the radial artery at the wrist under local anaesthesia. The wrist is numbed within minutes. The catheter — approximately 2mm in diameter — is threaded through the arterial system to the coronary artery under continuous X-ray guidance. You feel no pain during this journey because arteries contain no pain receptors.
Crossing the blockage: A fine guidewire is advanced through the narrowed segment of the coronary artery. This wire becomes the rail over which all subsequent equipment travels. Crossing a very tight blockage is often the most technically demanding step — requiring the precision and experience of an interventional cardiologist who has navigated hundreds of complex vessels.
Balloon dilation: A catheter with a deflated balloon at its tip is advanced to the blockage site. The balloon is inflated to high pressure — compressing the plaque against the artery wall and widening the lumen. This is the moment most patients expect to feel pain. They do not. The brief, controlled inflation is imperceptible.
Stent deployment: A stent — a precisely engineered metal mesh tube — is mounted on a second balloon catheter and advanced to the treated segment. When the balloon is inflated, the stent expands and is pressed firmly against the artery wall. The balloon is deflated and removed. The stent remains permanently, holding the artery open.
Result: Blood flows freely through the previously blocked segment. The oxygen starvation that was causing angina, breathlessness, or triggering a heart attack is resolved — immediately, within the same procedure.
For a thorough guide on understanding heart blockage symptoms and treatment options — including when angioplasty is appropriate versus when bypass surgery genuinely offers a superior outcome — our patient education library provides clear, evidence-based answers.
International cardiology guidelines support angioplasty as the preferred revascularisation strategy for:
Bypass surgery remains preferred for specific anatomical situations — unprotected left main disease with complex anatomy, severe three-vessel disease with high SYNTAX scores, or diabetes with diffuse multi-vessel involvement. Dr. Harshal Ingle discusses every case individually — no patient is pushed toward surgery without a thorough evaluation of whether angioplasty can achieve an equivalent result.
For heavily calcified coronary blockages, advanced intravascular treatments in Pune are not a premium add-on — they are a clinical necessity. Without them, standard angioplasty in calcified vessels fails silently, setting up the patient for a repeat procedure within months.
Calcium is the cardiologist’s most challenging adversary in the catheterisation laboratory. When plaque within the coronary artery wall mineralises over years — accelerated by diabetes, chronic kidney disease, and ageing — it creates a rigid, hardened shell around the vessel. Standard angioplasty balloons, no matter how high the inflation pressure, cannot reliably crack this calcium shell. The stent is deployed into a vessel that has never adequately dilated.
The result is predictable: an under-expanded stent with gaps between metal and wall — the precise conditions for turbulent blood flow, platelet activation, and eventual stent thrombosis or restenosis.
Intravascular Ultrasound (IVUS) is the first tool in the advanced angioplasty workflow for complex cases. A miniature ultrasound probe at the tip of a catheter captures cross-sectional images of the artery wall from inside as it is slowly withdrawn through the vessel.
IVUS measures:
This measurement-first approach transforms stent selection from estimation to precision engineering.
Optical Coherence Tomography (OCT) uses near-infrared light to generate images with resolution approximately 10 times sharper than IVUS. After the stent is deployed, OCT confirms:
According to a landmark study published in the AHA Journals on intravascular imaging outcomes, OCT-guided coronary intervention reduces major adverse cardiac events at one year by approximately 30–40% compared to angiography-guided procedures — driven by lower rates of stent thrombosis and target vessel revascularisation.
Explore the complete range of intravascular imaging guided angioplasty at Good Heart Clinic — including how IVUS and OCT are integrated into the procedural workflow for complex cases.
In cases where IVUS confirms severe circumferential calcification, the calcium must be physically modified before stenting. Two technologies serve this purpose at Good Heart Clinic:
Rotational Atherectomy (Rotablation): A diamond-tipped burr spinning at 150,000–180,000 RPM pulverises calcified plaque into microscopic particles that are safely absorbed into the bloodstream. The burr is advanced over the guidewire to the calcified segment and withdrawn multiple times until the calcium is adequately debulked.
Orbital Atherectomy: An eccentrically rotating diamond-coated crown modifies calcium in a larger circumferential arc. Dr. Harshal Ingle performed the first Orbital Atherectomy in Pune — expanding access to this technique for patients with the most complex calcified lesions in Maharashtra.
After calcium modification, standard balloon pre-dilation confirms adequate vessel preparation, and the stent is deployed into a properly prepared, adequately expanded artery — delivering the long-term result the patient needs.
A drug-eluting stent is permanent — it does not have an expiry date. With correct medication adherence and lifestyle management, a DES provides durable coronary artery patency that can last decades.
This is the question patients ask most urgently after a stent is placed — and it deserves a direct, honest answer rather than vague reassurance.
A bare-metal stent is a plain metal mesh that holds the artery open mechanically. As the artery heals around the stent, scar tissue (neointima) can form inside the stent, progressively narrowing the channel again — a process called in-stent restenosis, occurring in 20–30% of cases at one year.
A drug-eluting stent is coated with a polymer that slowly releases an antiproliferative drug — typically everolimus, zotarolimus, or sirolimus — directly into the artery wall at the stent site. This drug suppresses the scar tissue formation that causes restenosis. The result: in-stent restenosis rates fall to under 5–10% at one year in experienced, imaging-guided centres.
Current-generation ultrathin-strut DES have further improved on this — with strut thicknesses under 70 microns that minimise the vessel wall injury triggering restenosis in the first place.
The single most important determinant of stent longevity is Dual Antiplatelet Therapy (DAPT) — the combination of aspirin and a second antiplatelet agent (clopidogrel, ticagrelor, or prasugrel).
After a drug-eluting stent is placed:
Never stop antiplatelet medication without explicit guidance from your cardiologist — even for dental procedures, minor surgeries, or because you “feel fine.” This is the single most dangerous decision a post-stent patient can make.
| Timeline | What Must Happen |
|---|---|
| Day 1–7 post-procedure | DAPT daily. Wrist site care. No heavy lifting. |
| Week 2–4 | Return to light activity. Desk work. Follow-up visit. |
| Month 1 | Cardiology review — blood tests, medication assessment. |
| Month 3–6 | Stress test or clinical review depending on symptoms. |
| Month 12 | Annual cardiology review — reassess antiplatelet duration. |
| Year 2 onwards | Annual follow-up. Lipid panel. Blood pressure review. |
Lifestyle changes that protect the stent long-term:
The outcome of a coronary angioplasty procedure is determined before the stent is ever deployed — by the imaging technology used, the plaque preparation performed, and the cardiologist’s judgment in interpreting what the artery needs. At Good Heart Clinic, all three are operating at the highest available standard.
Dr. Harshal Ingle — MD (Medicine), DrNB Cardiology, Interventional Cardiologist at Ruby Hall Clinic, Pune — has performed over 1,000 complex coronary interventions including calcified lesions, bifurcations, multi-vessel disease, and left main angioplasties. His technical toolkit includes the full spectrum of intravascular imaging and plaque modification — IVUS, OCT, Rotablation, and Orbital Atherectomy — integrated into routine complex case management.
At most interventional centres in India, intravascular imaging is used selectively — in the most complex cases, or when the cardiologist suspects a problem. At Good Heart Clinic, imaging is integrated into the standard workflow for all complex lesions. The difference in long-term outcomes between “selective imaging” and “systematic imaging” is reflected directly in restenosis and repeat procedure rates.
When Dr. Ingle places a stent, the images confirm it before the procedure ends. That confirmation is what the 99.83% procedural success rate is built on.
Clinic credentials:
| Procedure | Approximate Cost (INR) |
|---|---|
| Coronary Angioplasty — Single Vessel (DES) | ₹1,20,000 – ₹2,00,000 |
| Multi-Vessel Angioplasty (2–3 vessels) | ₹2,00,000 – ₹4,00,000 |
| Angioplasty with IVUS Guidance | ₹1,50,000 – ₹2,80,000 |
| Angioplasty with OCT Guidance | ₹1,80,000 – ₹3,20,000 |
| Rotablation + Stenting (calcified lesion) | ₹2,00,000 – ₹3,50,000 |
| Orbital Atherectomy + OCT + Stenting | ₹2,50,000 – ₹4,50,000 |
| Post-procedure follow-up consultation | ₹500 – ₹1,500 |
What drives cost variation:
Insurance: Coronary angioplasty and stenting is covered under most mediclaim, corporate, and Ayushman Bharat (PMJAY) policies. Our team manages pre-authorisation from admission day — no last-minute paperwork.
A balloon catheter inserted through the wrist opens the blocked artery from inside, and a stent holds it open permanently. No chest incision, no general anaesthesia, no heart-lung machine. The entire procedure takes 30–90 minutes and most patients go home the same day or next morning.
For most single and double vessel blockages, and selected triple vessel cases, angioplasty delivers equivalent long-term outcomes to bypass surgery with significantly faster recovery and lower procedural risk. Bypass surgery remains preferred for specific anatomical patterns — left main disease with complex anatomy, or certain diffuse triple vessel disease in diabetics. Dr. Ingle assesses each case individually.
Calcified arteries resist standard balloon dilation — the stent under-expands and fails faster. IVUS and OCT measure calcium severity precisely, while Rotablation or Orbital Atherectomy pulverises the calcium before stenting. This preparation ensures the stent is fully expanded and correctly positioned — reducing restenosis risk dramatically.
A drug-eluting stent is permanent — it does not expire or degrade over time. With correct dual antiplatelet medication for 6–12 months and sustained lifestyle changes, it provides long-term arterial patency. Re-blockage rates are under 5–10% at one year in imaging-guided, experienced centres like Good Heart Clinic.
Dual antiplatelet therapy — aspirin plus clopidogrel, ticagrelor, or prasugrel — for a minimum of 6–12 months. Additionally: a statin for cholesterol, a beta-blocker for heart rate management, and an ACE inhibitor or ARB for blood pressure. Never stop any of these without direct guidance from your cardiologist.
Stopping dual antiplatelet therapy prematurely is the leading preventable cause of stent thrombosis — a sudden, complete clot inside the stent causing a major heart attack. Even missing one or two doses during the first 6 months carries meaningful risk. Always consult your cardiologist before adjusting any cardiac medication.
For complex, calcified, long, or bifurcation lesions — absolutely yes. Studies show imaging-guided angioplasty reduces the probability of major cardiac events at one year by 30–40% compared to angiography-only guidance. The upfront cost of imaging is far lower than the cost — financial and physical — of a repeat procedure 12–18 months later.
es. In-stent restenosis (re-narrowing inside a stent) is treated with a repeat balloon dilation, drug-coated balloon, or a second stent placed inside the first — all through the same wrist-access catheter approach. Stent thrombosis (sudden clotting) requires emergency angioplasty. Neither condition typically requires bypass surgery.
Single-vessel angioplasty with a drug-eluting stent costs approximately ₹1,20,000–₹2,00,000. Adding IVUS guidance brings the cost to ₹1,50,000–₹2,80,000. OCT-guided procedures range from ₹1,80,000–₹3,20,000. Complex calcified lesions requiring atherectomy cost ₹2,00,000–₹4,50,000. Most insurance policies cover these procedures.
Signs that Rotablation may be needed: heavy calcification visible on angiogram, prior balloon failure to fully expand, IVUS-confirmed calcium arc greater than 270 degrees, or a calcified lesion that a guidewire cannot easily cross. At Good Heart Clinic, IVUS assessment is performed before deciding on atherectomy — ensuring the decision is based on measured findings, not assumption.
A coronary artery blockage is not a life sentence. It is a diagnosis — and in 2025, with the imaging technology, plaque modification tools, and stent engineering available at Good Heart Clinic, it is a diagnosis that can be treated with precision, safety, and outcomes your family can rely on.
Coronary angioplasty in Pune at Good Heart Clinic is not the same procedure it was a decade ago. It is guided by images taken from inside your artery. It is delivered through the wrist. It is confirmed as optimal before you leave the procedure suite.
If you or someone in your family has been told they have a blocked coronary artery — whether mild, moderate, or severely calcified — bring that angiogram report to Dr. Harshal Ingle. The conversation that follows may be the most important one your heart has had.
Book your consultation today. Not because it is urgent. Because it is important.
Morning OPD — Cardiac OPD C7, Ground Floor, Building 3, Ruby Hall Clinic, Pune 411001 Evening OPD — 303A, Choice Apartments, Opp. Vohuman Cafe, Dhole Patil Road, Pune 411001 Appointments: 9822055445 / 8208950831 Cardiac Emergency: 9697020666 / 7722031119 goodheartclinic.com
OPD Timings: Monday to Saturday | Morning: 10 AM – 4 PM | Evening: 4 PM – 8 PM
We believe that every patient deserves absolute confidence in their care plan.
303, A, Choice Apartments Opp Vohuman Cafe , Dhole Patil Road , Pune
Support mail: drharshalingle@gmail.com
Opening Hours: Mon -Sat: 04.00 PM to 08.00 PM